|
In the ADR survey that we had discussed in detail last year, healthcare was the second biggest priority for people across India, across demographic groups. Voters indeed know their priorities right. Yet, this is the word cloud of issues that Republic TV, India’s most patriotic news channel discussed about during the election. Pakistan, Robert Vadra were some of the urgent topics. After that we heard a lot about Kashmir, Mandir and then CAA/NRC. I am sure Arnab Goswami must have owned the liberals many times during this period. While we were distracted by all the hot button topics, Indian healthcare was not getting the attention it deserved. Today there are few hospital beds left in major Indian cities due to COVID-19, and our doctors, especially resident doctors and nurses are overworked and underpaid. Tax payers are running from hospital to hospital in Delhi to save the lives of their loved ones. Imagine if ours was a civil polity where the people‘s concerns were actually heard. Where a primary priority of our government was also health capacity. And where people were not dosed with talking points that politicians and their surrogates wanted you to talk about. People love conspiracy theories, and so here is a real conspiracy theory for you: you are being mind controlled by those in power through the black mirrors (TV, smartphones) every single day. They shape your agenda, when their agenda should be shaped by you. 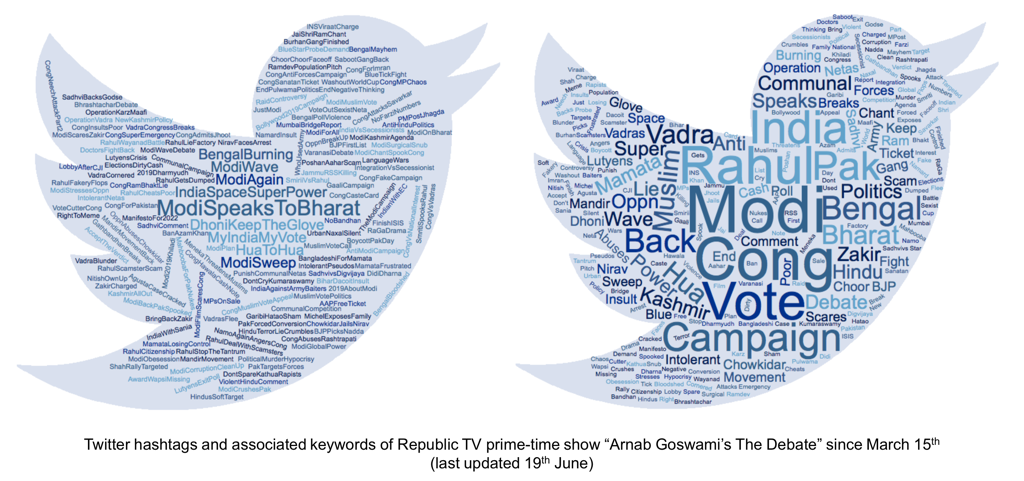
1 Comment
The Indian stimulus package offers around 0.55% of the GDP (around Rs 1.1 lack crore) as immediate measures for the poor, in which 0.31% of the GDP is in-kind transfers, most of which were offered on 26th March 2020. May month measures did not offer substantial relief for the immediate needs of the poor. The economic stimulus packages being offered in response to the COVID-19 crisis, are like a fruit basket with a motley of measures. Each measure is different, based on the intended beneficiary, the level of immediacy and the instrument of relief. This article identifies stimulus measures announced by the Indian government where the poor or their employers are direct beneficiaries, and which are intended to immediately provide them relief. Direct in-kind measures: The largest stimulus measure by the Indian government was announced on 26th March 2020, a day after the beginning of the lockdown. It provided 800 million poor individuals with 5 kg of wheat/rice per month, and 1 kg of pulses per household per month, for three months. The total fiscal cost of this measure was estimated to be Rs 45000 crore (USD 6 billion). A follow up to this scheme was announced on 14th May 2020 when 80 million migrant workers - including those who did not have proper identification - were included in the scheme (for 2 months) at a stated fiscal cost of Rs 3500 crore (USD 467 million). In a related measure the government also announced on 26th March 2020 a provision of LPG cylinders for 3 months to 80 million households, at a fiscal cost of Rs 13000 crore (USD 1.73 billion). These in-kind transfers worth Rs 61500 crore (USD 8.2 billion) are welcome measures that are providing necessary relief to hundreds of millions Indians. Based on the 26thMarch announcements, per capita, a poor person was promised grain transfers worth (cost to government) Rs 560 (USD 7.5), and a poor household was promised an LPG transfer worth Rs 1625 (USD 22). Of course, for a program of such a scale, there have also been leakages in the implementation of this relief, due to lack of accessibility or endemic corruption, an example of which has been reported in Jharkhand. Direct cash measures: Along with the in-kind transfers, specific vulnerable groups have been provided direct cash and income transfers. These beneficiaries include 204 million women who receive Rs 1500 (USD 20 in three monthly instalments) through their Jan Dhan Bank accounts at a fiscal cost of Rs 30600 crore (USD 4.08 billion). 30 million poor widows, senior citizens and disabled receive a one-time payment of Rs 1000 (USD 13) at a fiscal cost of Rs 3000 crore (USD 400 million). 7.2 million workers with a monthly income of less than Rs 15000 (USD 200) in firms with fewer than 100 employees, get 24% of their monthly salary paid by the government for 3 months, at an expected fiscal cost of Rs 2800 crore (USD 373 million)1. This scheme was further extended for 3 more months at a stated fiscal cost of Rs 2800 crore (USD 373 million). The government has also made a wage increase of Rs 20 (USD 0.27) per day for MNREGA workers helping 136 million individuals at a fiscal cost of Rs 5600 crore (USD 747 million). Although these transfers are worth Rs 39200 crore (USD 5.2 billion), the size of relief per capita is very small. For example the three Rs 500 per month instalments to 204 million women is inadequate to provide a sizeable relief. A paucity of cash has important negative ramifications on local demand, and as a consequence on the local economies. Hence, helping the poor through cash may be an important step in reviving local economies. Other direct measures: Additionally the government has promised to create a fund for stressed MSMEs with a stated commitment of credit guarantee of Rs 4000 crore (USD 533 million), helping 200 thousand MSMEs. This is a welcome measure to help small businesses and their employees in distress. Other measures: To help urban migrant workers the government, on 26th March 2020, directed state governments to utilise Rs 31000 crore (USD 4.1 billion) of the existing welfare fund for building and construction workers, to help 35 million workers enrolled in the fund. This fund helped state governments finance their relief measures. However a report by SWAN (Stranded Workers Action Network) showcased that even after 32 days of lockdown 97% of the migrants they surveyed had not received cash relief, 82% had not received food grains, and 68% did not have access to cooked meals. The government plans to provide an advance payment of Rs 2000 (USD 260 million) to 87 million farmers who are part of the PM-Kisan Yojana, which incurs no additional fiscal cost. 30 million small and marginal farmers are also expected to receive additional working capital through NABARD which will lead to cash infusion of RS 30000 crore (USD 4 billion). Similarly the government promises to provide working credit of up to Rs 10000 (USD 133) to 5 million street vendors leading to cash infusion of Rs 5000 crore (USD 666 million). A similar mega measure of credit infusion has been offered to 4.5 million MSMEs leading to cash infusion of Rs 200000 crore (USD 26.7 billion), helping them stay afloat saving jobs. Each of these measures, although incur no fiscal cost on the governments, are welcome steps to provide relief to small businesses, employees, micro entrepreneurs, and workers for survival. Summary The overall fiscal cost of the stimulus package for immediate relief to the poor is about Rs 110300 crore (USD 14.7 billion), that amounts to around 0.55% of the GDP in which 0.31% of the GDP is in-kind transfers. The overall stimulus is estimated by various agencies to have a fiscal cost of around 1% and it is encouraging to see that more than half of those fiscally costly measures are directed for the poor. Yet it is also worth noticing that most of these measures for the poor were already announced on 26th March 2020. In fact, in the much awaited wave of “self-reliant India” announcements in May, only three measures with a fiscal cost of Rs 10300 crore (USD 1.37 billion), were of direct relevance to the poor, although a variety of credit infusion measures were taken to help businesses that employ them. Hence, the second wave of announcements in the month of May have been a lost opportunity for providing more immediate relief to the poor. Given the scale of India’s poverty, severity of its lockdown, and the bullish growth prospects in the long term, there is space for more spending on the poor, which the government should focus on. (This article appeared on IIMB’s faculty blog on 2nd June 2020.)
Resident doctors are fighting the war against the COVID-19 crisis from the front lines. There is no dearth of showering of wordy and flowery gratitude for all their hard work and efforts.
Young doctors in their early 30s, who chose the path of being a doctor over other lucrative careers, are earning between Rs 40000 to 50000 a month as residents, while doing frontline COVID-19 duty, exposing themselves to all the risks, with no hazard pay. If they wanted to leave after the crisis, to pursue a better career, they would be asked to pay a hefty bond in some states, such as West Bengal. On top of all this, there are reports from around India that resident doctors are being treated poorly (without basic equipment) with reports of their pay being cut or docked in some instances. If such is the working conditions and pay incentives of top of the line resident doctors in their early 30s, what is the incentive left in this country for people to become a doctor? For a country that has abysmally low doctors per capita, such a poor incentive structure does not make the medical career any more lucrative, and the future of healthcare in India any more assuring. Today if you want to pursue a well-paid career, a generic MBA seems to be a must. Opportunities for those who pursue expertise, in science and especially in medicine are meager. For someone in their 20s and 30s, being a YouTube “influencer” offers a more attractive career path than being a doctor. There is something broken about our economic system when being a highly educated scientist or a doctor is not a lucrative early career option, of the same kind as a bureaucrat, a consultant, or a Twitter troll! Why are doctors, even those with decent medical experience in their 30s, treated as low paid “residents” when clearly they are qualified experts. Are they less capable, less intelligent, less hard-working, less rare, less essential professionals than the bureaucrats? The skills of Indian doctors are highly valued across the world. Then why can’t India value its own? Its true that bureaucrats in India are also paid only modest salaries, but they are afforded certain benefits which make their jobs lucrative to many including from the private sector. They are treated as babus, when resident doctors of their age are given little voice, neither within the profession nor outside. Why do young doctors not get comparable benefits? Why can’t all the Indian doctors above a certain qualification, serving public healthcare, be enlisted in a national medical service (similar to the UPSC) and be afforded a decent seventh pay commission package that matches the depth of their expertise? This is also a recent request that the Federation of Resident Doctors' Association India (FORDA) has made to the Prime minister. Being a doctor is a social service, and they understand that such a service does come with some sacrifices. They are doing their job out of a sense of duty, not for the greed of money. Hence, doctors do not expect hedge fund manager salaries. But a good salary, a good package with a decent quality of life - what stops the government from offering them so? A major reason why paying generous salaries to the doctors, especially those who are young, doesn't cross the mind of Indian policymakers is because human capital - health and education - seems to have been a historical low priority of the nation. India’s government spends around 1% of the GDP on health (lowest among G20 countries), when China spends around 3%, the USA over 14%, the UK around 7.5%, and Brazil around 4%. 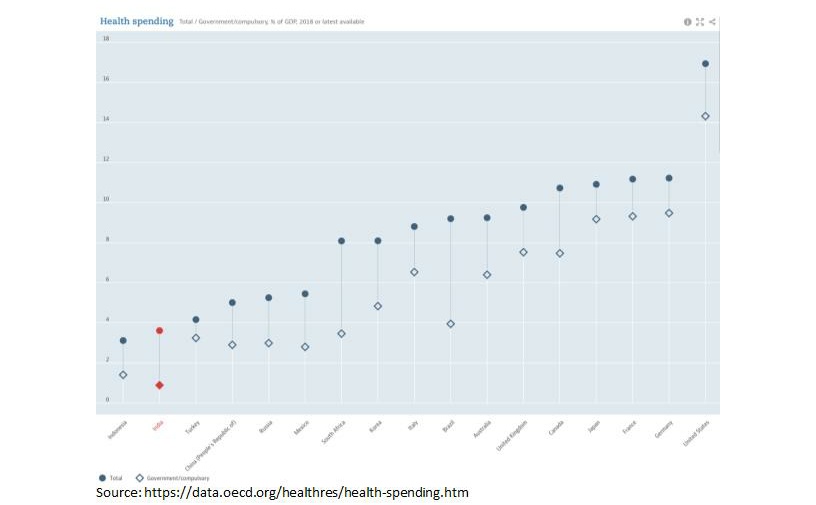 When there exists such a small kitty for health, is it a wonder that a pay raise for doctors never reaches the decision desk? At the same time, lack of private competition in the health industry further worsens the situation because doctors have no labor mobility. They work effectively within a government monopoly. While we can debate how much privatization should there be in Indian healthcare; yet the fact that competitive salaries must be paid to the doctors is a no brainer. The condition of Indian resident doctors is also a reflection on the state of human development in India. Human capital in India has been ignored, first in favor of top-down industrialization during the pre liberalization era, and then of pro-business privatization in the liberalization era. Where are the much-needed investments in public goods? Even the much-anticipated stimulus package speaks the language of supply-side economics, ignoring the obvious fact that the coronavirus pandemic is primarily a health crisis, and a priority for the government must be to invest more in public goods such as healthcare. The machines, the factories, the bridges, and other “temples” have been given a priority in the country for far too long over the doctors, the teachers, the nurses, and the scientists, i.e. the actual skilled class of the country that holds it together. As human capital has been ignored, no wonder India has uncharacteristically low levels of human development: infant mortality is high, literacy rates are low, drop out rates continue to be up, and life expectancy still remains 10 years behind China. We should hope that at least after the pandemic, our investment in public health will go up. For sustainable growth, a simple one-dimensional focus on businesses and capital won't be fruitful, and it will require a holistic approach. The pandemic is an opportunity for this understanding - of the importance of public health - to dawn. In the latest stimulus package the government has given an indication of increasing health expenditure, but the amount or percentage GDP terms were not specified. A significantly greater fraction of India’s GDP must go into healthcare. And with such an increase, the health workers, including doctors should get the respect, recognition, privileges, and the pay that they deserve. (This article appeared on IIMB’s faculty blog on 19th May 2020.) |
Prateek RajPersonal blog. Views expressed are my own, expressed in personal capacity. Archives
May 2021
Categories |
||
 RSS Feed
RSS Feed
